Overview

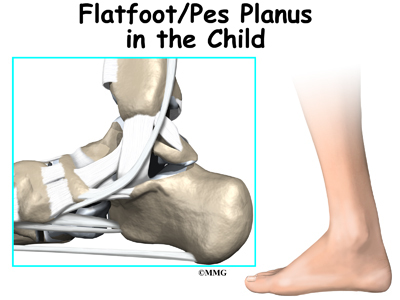
Feet usually have an arch on the inside portion of the foot. A flat foot is a foot that has lost or never developed this arch. It is often associated with the lower part of the legs being angled outwards. Most flat feet are flexible. This type rarely causes problems and usually do not require treatment. Rigid flat feet can cause problems and are best treated.
Causes
The most common acquired flat foot in adults is due to Posterior Tibial Tendon Dysfunction. This develops with repetitive stress on the main supporting tendon of the arch over a long period of time. As the body ages, ligaments and muscles can weaken, leaving the job of supporting the arch all to this tendon. The tendon cannot hold all the weight for long, and it gradually gives out, leading to a progressively lower arch. This form of flat foot is often accompanied by pain radiating behind the ankle, consistent with the course of the posterior tibial tendon. Compounding matters is the fact that the human foot was not originally designed to withstand the types of terrain and forces it is subjected to today. Nowhere in nature do you see the flat hard surfaces that we so commonly walk on in present times. Walking on this type of surface continuously puts unnatural stress on the arch. The fact that the average American is overweight does not help the arch much either-obesity is a leading cause of flat feet as the arch collapses under the excessive bodyweight. Furthermore, the average life span has increased dramatically in the last century, meaning that not only does the arch deal with heavy weight on hard flat ground, but also must now do so for longer periods of time. These are all reasons to take extra care of our feet now in order to prevent problems later.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
fallen arches shoes
Non Surgical Treatment
Custom orthotics are specially designed insoles, which are made for your by prescription. This is done by taking a plaster cast of the foot in its neutral position and is then sent to a laboratory, with your prescription to be made to your exact specifications. The insole then correctly aligns your foot and as a result your body. This will relieve abnormal strain of tissues and structures which can cause pain. For less severe mal-alignments or for sports use a wide variety of temporary insoles.
Surgical Treatment
Since there are many different causes of flatfoot, the types of flatfoot reconstruction surgery are best categorized by the conditions. Posterior tibial tendon dysfunction. In this condition, the tendon connecting the calf muscle to the inner foot is torn or inflamed. Once the tendon is damaged it no longer can serve its main function of supporting the arch of the foot. Flatfoot is the main result of this type of condition and can be treated by the following flatfoot reconstruction surgeries. Lengthening of the Achilles tendon. Otherwise known as gastrocnemius recession, this procedure is used to lengthen the calf muscles in the leg. This surgery treats flatfoot and prevents it from returning in the future. This procedure is often combined with other surgeries to correct posterior tibial tendon dysfunction. Cleaning the tendon. Also known as tenosynovectomy, this procedure is used in the earlier and less severe stages of posterior tibial tendon dysfunction. It is performed before the arch collapses and while the tendon is only mildly affected. The inflamed tissue is cleaned away and removed from the remaining healthy tendon. Tendon transfer. This procedure is done to correct flatfoot and reform the lost arch in the foot. During the procedure, the diseased tendon is removed and replaced by tendon from another area of the foot. If the tendon is only partially damaged, the inflamed part is cleaned and removed then attached to a new tendon. Cutting and shifting bones. Also called an osteotomy, this procedure consists of cutting and reconstructing bones in the foot to reconstruct the arch. The heel bone and the midfoot are most likely reshaped to achieve this desired result. A bone graft may be used to fuse the bones or to lengthen the outside of the foot. Temporary instrumentation such as screws and plates can also be used to hold the bones together while they heal.
Prevention
Flatfeet in children are often an inherited family trait, but it may be possible to prevent the condition in some cases. Recent research has shown that there are several social or cultural factors that can cause flatfeet. These factors include the following, obesity, overweight, unnecessary orthopedic treatments, wearing rigid shoes at a young age, In 1992, a study in India of 2300 children aged 4-13 demonstrated a significant difference in the rate of flatfeet among those who wore shoes regularly and those who did not. In this study, wearing inflexible, closed-toe shoes in early childhood was shown to have a negative effect on the normal development of arches. Children who were allowed to go barefoot or who wore light sandals and slippers had a much lower rate of flatfeet. In 1999, a study in Spain of 1181 children aged 4-13 revealed that the use of orthopedic shoes for treatment of flatfeet in children not only failed to correct the problem, but actually worsened the condition by preventing the normal flexing and arch development of bare or lightly protected feet. Finally, in 2006, a study of 835 children aged 3-6 showed significant differences in the rate of flatfeet based on weight, with normal-weight children having lower rates of flatfeet than children who were overweight or obese. Among adults, flatfeet due to injury, disease, or normal aging are not preventable. However, when flatfeet are related to lifestyle factors, such as physical activities, shoe selection, and weight gain, careful attention to these factors may prevent the development of flatfeet.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
Feet usually have an arch on the inside portion of the foot. A flat foot is a foot that has lost or never developed this arch. It is often associated with the lower part of the legs being angled outwards. Most flat feet are flexible. This type rarely causes problems and usually do not require treatment. Rigid flat feet can cause problems and are best treated.
Causes
The most common acquired flat foot in adults is due to Posterior Tibial Tendon Dysfunction. This develops with repetitive stress on the main supporting tendon of the arch over a long period of time. As the body ages, ligaments and muscles can weaken, leaving the job of supporting the arch all to this tendon. The tendon cannot hold all the weight for long, and it gradually gives out, leading to a progressively lower arch. This form of flat foot is often accompanied by pain radiating behind the ankle, consistent with the course of the posterior tibial tendon. Compounding matters is the fact that the human foot was not originally designed to withstand the types of terrain and forces it is subjected to today. Nowhere in nature do you see the flat hard surfaces that we so commonly walk on in present times. Walking on this type of surface continuously puts unnatural stress on the arch. The fact that the average American is overweight does not help the arch much either-obesity is a leading cause of flat feet as the arch collapses under the excessive bodyweight. Furthermore, the average life span has increased dramatically in the last century, meaning that not only does the arch deal with heavy weight on hard flat ground, but also must now do so for longer periods of time. These are all reasons to take extra care of our feet now in order to prevent problems later.
Symptoms
Many people have flat feet and notice no problems and require no treatment. But others may experience the following symptoms, Feet tire easily, painful or achy feet, especially in the areas of the arches and heels, the inside bottom of your feet become swollen, foot movement, such as standing on your toes, is difficult, back and leg pain, If you notice any of these symptoms, it's time for a trip to the doctor.
Diagnosis
Many medical professionals can diagnose a flat foot by examining the patient standing or just looking at them. On going up onto tip toe the deformity will correct when this is a flexible flat foot in a child with lax joints. Such correction is not seen in the adult with a rigid flat foot. An easy and traditional home diagnosis is the "wet footprint" test, performed by wetting the feet in water and then standing on a smooth, level surface such as smooth concrete or thin cardboard or heavy paper. Usually, the more the sole of the foot that makes contact (leaves a footprint), the flatter the foot. In more extreme cases, known as a kinked flatfoot, the entire inner edge of the footprint may actually bulge outward, where in a normal to high arch this part of the sole of the foot does not make contact with the ground at all.
fallen arches shoes
Non Surgical Treatment
Custom orthotics are specially designed insoles, which are made for your by prescription. This is done by taking a plaster cast of the foot in its neutral position and is then sent to a laboratory, with your prescription to be made to your exact specifications. The insole then correctly aligns your foot and as a result your body. This will relieve abnormal strain of tissues and structures which can cause pain. For less severe mal-alignments or for sports use a wide variety of temporary insoles.
Surgical Treatment
Since there are many different causes of flatfoot, the types of flatfoot reconstruction surgery are best categorized by the conditions. Posterior tibial tendon dysfunction. In this condition, the tendon connecting the calf muscle to the inner foot is torn or inflamed. Once the tendon is damaged it no longer can serve its main function of supporting the arch of the foot. Flatfoot is the main result of this type of condition and can be treated by the following flatfoot reconstruction surgeries. Lengthening of the Achilles tendon. Otherwise known as gastrocnemius recession, this procedure is used to lengthen the calf muscles in the leg. This surgery treats flatfoot and prevents it from returning in the future. This procedure is often combined with other surgeries to correct posterior tibial tendon dysfunction. Cleaning the tendon. Also known as tenosynovectomy, this procedure is used in the earlier and less severe stages of posterior tibial tendon dysfunction. It is performed before the arch collapses and while the tendon is only mildly affected. The inflamed tissue is cleaned away and removed from the remaining healthy tendon. Tendon transfer. This procedure is done to correct flatfoot and reform the lost arch in the foot. During the procedure, the diseased tendon is removed and replaced by tendon from another area of the foot. If the tendon is only partially damaged, the inflamed part is cleaned and removed then attached to a new tendon. Cutting and shifting bones. Also called an osteotomy, this procedure consists of cutting and reconstructing bones in the foot to reconstruct the arch. The heel bone and the midfoot are most likely reshaped to achieve this desired result. A bone graft may be used to fuse the bones or to lengthen the outside of the foot. Temporary instrumentation such as screws and plates can also be used to hold the bones together while they heal.
Prevention
Flatfeet in children are often an inherited family trait, but it may be possible to prevent the condition in some cases. Recent research has shown that there are several social or cultural factors that can cause flatfeet. These factors include the following, obesity, overweight, unnecessary orthopedic treatments, wearing rigid shoes at a young age, In 1992, a study in India of 2300 children aged 4-13 demonstrated a significant difference in the rate of flatfeet among those who wore shoes regularly and those who did not. In this study, wearing inflexible, closed-toe shoes in early childhood was shown to have a negative effect on the normal development of arches. Children who were allowed to go barefoot or who wore light sandals and slippers had a much lower rate of flatfeet. In 1999, a study in Spain of 1181 children aged 4-13 revealed that the use of orthopedic shoes for treatment of flatfeet in children not only failed to correct the problem, but actually worsened the condition by preventing the normal flexing and arch development of bare or lightly protected feet. Finally, in 2006, a study of 835 children aged 3-6 showed significant differences in the rate of flatfeet based on weight, with normal-weight children having lower rates of flatfeet than children who were overweight or obese. Among adults, flatfeet due to injury, disease, or normal aging are not preventable. However, when flatfeet are related to lifestyle factors, such as physical activities, shoe selection, and weight gain, careful attention to these factors may prevent the development of flatfeet.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.

 Neuromas are generally benign or non-cancerous growths of nerve tissue, developing in various parts of the body. Morton?s Neuromas are confined to the nerves of the foot, most commonly, between the third and fourth toes. The condition involves a thickening of the tissue around one of the digital nerves leading to the toes and does not qualify as an actual tumor. The affliction causes a sharp, burning pain, usually in the region of the ball of the foot. A patient?s toes may also sting, burn or exhibit numbness. Often, the symptoms have been likened to ?walking on a marble.?
Neuromas are generally benign or non-cancerous growths of nerve tissue, developing in various parts of the body. Morton?s Neuromas are confined to the nerves of the foot, most commonly, between the third and fourth toes. The condition involves a thickening of the tissue around one of the digital nerves leading to the toes and does not qualify as an actual tumor. The affliction causes a sharp, burning pain, usually in the region of the ball of the foot. A patient?s toes may also sting, burn or exhibit numbness. Often, the symptoms have been likened to ?walking on a marble.?


 Overview
Overview Symptoms
Symptoms Prevention
Prevention Overview
Overview

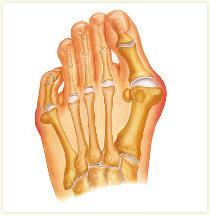 Bunions (hallux valgus) are often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. With a bunion, the big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion's "bump." Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which continues to become increasingly prominent. Bunions can be painful, but not always. Bunions are always progressive, so the deformity becomes more prounced over time, even if its not painful.
Bunions (hallux valgus) are often described as a bump on the side of the big toe. But a bunion is more than that. The visible bump actually reflects changes in the bony framework of the front part of the foot. With a bunion, the big toe leans toward the second toe, rather than pointing straight ahead. This throws the bones out of alignment, producing the bunion's "bump." Bunions are a progressive disorder. They begin with a leaning of the big toe, gradually changing the angle of the bones over the years and slowly producing the characteristic bump, which continues to become increasingly prominent. Bunions can be painful, but not always. Bunions are always progressive, so the deformity becomes more prounced over time, even if its not painful.
